What is incident reporting system in healthcare? Patient Incident Types Harmful Incident. A harmful incident in injury or illness to a patient or another person. For example, a patient. A near miss is when there was potential harm to a patient or another person was almost harmed but the.
Health organizations have a responsibility to learn from health-care-associated harm.

Almost immediately, several health systems responded to this call. Most of these health systems ha at the core of their mission, a commitment to learn from medical errors and adverse events. Most subsequently set up systems to report and learn from so-called patient-safety incidents. One assumed that such systems would facilitate both the identification of systemic weaknesses that contribute to errors in health care and the learning necessary to prevent such errors recurring.
However, in contrast to some other high-risk industries, where learning from accidents, mistakes and system failures appears to have led to major improvements in safety,2little evidence exists that such systems have led to general reductions in the incidence or severity of patient-safety incident. See full list on who. We searched the research literature for studies published before that had used a framework, system or taxonomy for the classification of harm severity in patient-safety incidents occurring in primary care.
Two reviewers searched databases to find research studies and systematic reviews that had covered patient-safety incidents in primary care.
Disagreements over inclusion were resolved via arbitration by a third reviewer. We based the searches on, and used the same search terms an. We carried out a framework analysis of the content of each of the classification systems, to identify the key themes an particularly, each system’s strengths and weaknesses relative to WHO’s International Classification. We especially focused on the range of characteristics used to define harm. Encompassing both a-priori and emerging concepts, framework analysis facilitates the development of a themed matrix by organizing and managing data through a process of summation.
We used the of the framework analyses in developing our new classification system, through an iterative process. Together, we have experience in coding and analysing over 60 0reports of patient-safety incidents in primary care for several mixed-methods research studies. We discussed the common and novel features of each classification system and considered the practicalities of identifying such characteristics when coding incidents that had occurred during primary care. We named our new system the Primary Care Harm Severity Classification System.
Table provides examples, from reports collected by the United Kingdom’s National Reporting and Learning System, of patient-safety incidents that would be assigned to each of the new system’s categories of harm severity. We used the insights gained from the process of applying the new classification system to real examples of patient-safety incidents to inform the concepts and definitions used in the new system (Box 2), which offer guidance to future users of the system. Definitions of harm severity vary greatly between existing classification systems for patient-safety incidents in primary care.
In general, the adverse effects of hospitalization and psychological harm have previously been neglected. Health-care organizations need a consistent and reliable way of knowing which aspects of their care result in the most harm to patients. Advances in the methods of analysis of incident reports from primary-care facilities should facilitate the scoping of action to reduce risk and improve patient safety, including the planning for research that could lead to more effective interventions. Our new classification system for harm severity is a starting point for a learning process that should lead from the more effective anal.
The effective application of any system for classifying the severity of harm associated with patient-safety incidents depends on judgments made by the individuals coding the incidents.
Such judgements will vary depending on each coder’s clinical role, level of clinical knowledge and past experiences. In this paper, we have mapped out the key constructs for inclusion in an appropriate framework for classifying the severity of harm associated with patient-safety incidents in primary care. Given the broad range of events described in incident reports, the wide scope of the definitions we use is intentional. Although a lengthier and more prescriptive classification system may achieve greater consistency between users, it risks being too complex to use in practice and too reductionist to support useful interpretation and learning.
In the future, we plan to undertake a validation study in which a diverse, multidisciplinary panel of primary-care professionals, researchers and patient advoc. Previous attempts to identify and learn from the most important sources of harm to patients in primary care have been restricted by the lack of a universal standard system for classifying the severity of such harm and the general neglect of psychological harm in this context. Health-care leaders must develop robust mechanisms for generating useful reports of patient-safety incidents and acting on those reports to improve patient safety. We have empirically developed a new classification system that has the potential to be applied internationally, across primary-care settings, to improve the detection and prevention of incidents that cause the most severe harm to patients. We thank H Prosser Evans, A Cooper, F Smith, R Samiurwo, A Omar, R Watson, P Paul and A Chuter.
GP has a dual appointment with Harvard Medical School, Boston, USA. AC-S has a dual appointment, as honorary professor, with the Australian Institute of Health Innovation, Macquarie University, Sydney, Australia. The Joint Commission and the Centers for Medicare and Medicaid Services mandate that facilities have a way to track adverse events. Some states also have reporting requirement for certain types of adverse events.
It was about understanding what could be a potential professional liability claim. You wanted to track incidents to enable. Over the past years, we’ve been enhancing our system, and it now includes incident reporting, claims management, complaints and grievances, and worker’s comp as well as quality events, peer revi. In most cases, incident reporting is part of the hospital’s overall IT structure.
Some facilities are still using paper forms to collect the initial data but, as we’ve seen, that will soon change due to added requirements for computerization. As more hospitals move to fully computerized forms and point-of-service data entry, training and education will help smooth the transition. Medical Interactive Community LLC, a two-year-old company in Metairie, Louisiana, is a provider of online risk man.
I believe the major issue today is not with incident reporting itself, but with taking action on the reported data in order to truly affect change. These are the words of Catherine Lathem, vice president of product management at RL Solutions, Toronto, Canada. CRG Medical, a technology company in Houston, Texas, developed the award-winning “Purple Button,” an AHRQ Common Formats mobile application that enables healthcare providers to visualize data in the KBCore hazard detection and early-warning database through predefined reports. Clinicians are able to capture and share patient safety knowledge in seconds.
Many of the developed countries of the world have government-run or -supported healthcare. This is certainly true in Britain and Canada. Mike Weber, director of product management and safety solutions at Quantros, hasn’t seen a great impact from the Affordable Care Act (ACA) yet. We think it is coming, especially with Medicare and Medicaid.
Facilities will need to be part of a PSO, a patient safety organization. Some of the regulations within the P. A report has two functions: It informs the administration of the incident so management can prevent similar incidents in the future. The employee incident report varies according to the type of incident being reported. The initial incident report is the first step in the incident investigation process no matter what type of incident is being recorded. An effective event reporting system should have four key attributes: While traditional event reporting systems have been paper base technological enhancements have allowed the development of Web-based systems and systems that can receive information from electronic medical records.
Specialized systems have also been developed for specific settings, such as the Intensive Care Unit Safety Reporting System and systems for reporting surgical and anesthesia-related errors. The advantages of voluntary event reporting systems include their relative acceptability and the involvement of frontline personnel in identifying safety hazards for the. Voluntary event reporting systems need not be confined to a single hospital or organization. The limitations of voluntary event reporting systems have been well documented. Event reports are subject to selection bias due to their voluntary nature.
Compared with medical record review and direct observation, event reports capture only a fraction of events and may not reliably identify serious events. The spectrum of reported events is limite in part due to the fact that physiciansgenerally do not utilize voluntary event reporting systems. Source: Evans SM, Berry JG, Smith BJ, et al. Attitudes and barriers to incident reporting: a collaborative hospital study. Box) and concluded that according to these standards, most hospitals do not maintain effective event reporting systems.
In addition to lack of physician reporting, most hospitals surveyed did not have robust processes for analyzing and acting upon aggregated event. Qual Saf Health Care. While event reporting utilization can be a marker of a positive safety culture within an organization, organizations should resist the temptation to encourage event reporting without a concrete plan for following up on reported events. A PSNet perspectivedescribed a framework for incorporating voluntary event reports into a cohesive plan for improving safety.
The framework emphasizes analysis of the events and documenting process improvements arising from event analysis, rather than encouraging event reporting for its own sake. Health care providers may choose to work with a PSO and specify the scope and volume of patient safety information to share with a PSO. Because health care providers can set limits on the ability of PSOs to use and share their information, this system does not follow the pattern of traditional voluntary reporting systems. However, health care providers and PSOs may aggregate patient safety event information on a voluntary basis, and AHRQ will establish a network of patient safety databases that can receive and aggregate nonidentifiable data that are submitted voluntarily.
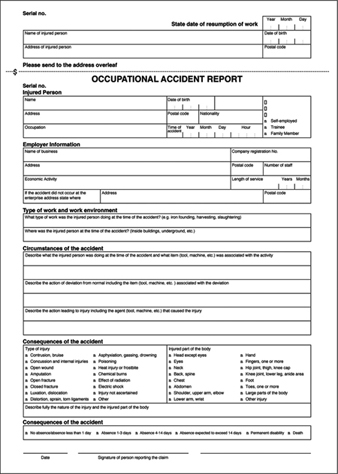
AHRQ has also developed Common Formats—standardized definitions and reporting format. In a health care facility, such as a hospital, nursing home, or assisted living, an incident report or accident report is a form that is filled out in order to record details of an unusual event that occurs at the facility , such as an injury to a patient. The HIPAA definition of a security incident is, “the attempted or successful unauthorized access, use, disclosure, modification, or destruction of information or interference with system operations in an information system. The HIPAA Security Rule requires covered entities and business associates to “implement a policy and procedures to address security incidents.
The Privacy Rule (and Section 16of the Omnibus Rule) requires the organization to report Breaches of Protected Health Information. Both Rules start with an assumption that healthcare organizations know an incident has occurred. Therefore, incident management procedures should include initial discovery and reporting of suspected incidents, or events, as the first step.
One challenge in building a reporting process is to quickly alert individuals who are authorized to validate and respond to an incident. Unfortunately, functional stovepipes may build independent incident structures leading to separate security, privacy, technical, and non-technical reporting processes. This fosters an environment with training challenges and reporting delays. In response, healthcare organizations should consider one incident reporting and analysis process. A single process simplifies workforce training, facilitates early executive and compliance alerting, and br.
Just as not all events can be validated to be incidents, not all incidents reach the threshold to be called breaches. The analysis of a suspected breach and application of the defined exclusions are challenging for even experienced compliance teams. The Omnibus Rule goes on to define a set of exclusions to the term breach. Therefore, the use of the term breach should be limited to only those incidents that have thoroughly been reviewed and found to meet the strict breach definition contained in the HIPAA regulations. The authority to declare a breach should therefore be limited to a very small group of individuals who have been granted authority to perform the evaluation and the competence to evaluate the.
Many healthcare providers are required to have a compliance hotline. These hotlines provide whistleblowers an outlet to report compliance issues without fear of identification or retribution. To work properly, all members of the workforce must be trained and retrained on how to report issues.
Healthcare organizations with an anonymous incident reporting hotline will likely experience a higher number of incidents that those without a hotline, but this is a positive situation. Incident reporting processes can benefit from similar processes and protections. Compliance and IT professionals cannot manage what they don’t measure, and underreporting security and privacy events creates a false sense of security and lead to under investment. The anonymous reporting portal will facilitate a higher reporting frequency, but only as long as the workforce feels comfortable that retribution is not tolerated. Therefore, leaders should not tolerate retribution, or else incidents will be underreporte.
In summary, healthcare organizations can benefit from a detailed incident policy that starts at a suspected discovery, through the closure. There should be one reporting process that quickly alerts trained responders. Finally, organizations that use third parties for helping build and test procedures fare better because of the cross-functional, cross-organizational lessons learned.
It will also be beneficial to have these same third parties help by retaining individuals who have been tested in other situations. Clyde Hewitt is vice president of security strategy at CynergisTek. He brings more than years of executive leadership experience in cybersecurity to his position with CynergisTek, where his many responsibilities include being the senior security advisor and client executive, thought leader and developer of strategic direction for information and cybersecurity services, nationwide business development lead for security services, and contributor to CynergisTek’s industry out. While there are many different healthcare dashboards, each is an analytical, comprehensive, and dynamic tool that provides a condense visual report of key performance indicators (KPIs). Presenting metrics in such a manner makes it easier to understand progress and challenges, and gives a high-level snapshot of what’s going on in your facility.
Instant Downloa Mail Paper Copy or Hard Copy Delivery, Start and Order Now! Here are three different incident report forms for you and try to fill in by yourself. When you do this, please bear all the rules above in mind. Laboratory Incident Report.
Hospital Incident Report. An incident report should be filed whenever an unexpected event occurs. The rule of thumb is that any time a patient makes a complaint, a medication error occurs, a medical device malfunctions, or anyone—patient, staff member, or visitor—is injured or involved in a situation with the potential for injury, an incident report is required. However, the actual value of these systems is increasingly subject to debate.
Reporting systems, both local and national, are overwhelmed by the volume of reports and fall short in defining recommendations. Overview PSOs are required to collect and analyze data in a standardized manner. An ambulance report not being fully completed.
Documentation – no access to. Examples Notes not arriving when a patient changes their GP. Behavioral Health reportable adverse incidents include, but are not limited to, the following: Any death (include cause of death if known) Any absence without authorization (AWA) Any serious injury resulting in hospitalization. Any sexual assault or alleged sexual assault. However, falls and decubitus ulcers are visible ha (outcomes) that might have resulted from failure to monitor patients or an inaccessible bedpan atient rms 5. How to Write an Incident Report It’s important to establish a systematic method for investigating incidents.
It’s also equally important to have a report prepared that enables you to record every relevant aspect of the incident –this is the essential first step in the incident reporting process.